


This article is free to read. So is every article Electric Literature publishes. No limits, no paywalls—now or ever. Support from readers like you makes that possible.
Electric Literature is proud to be a space where writers are always paid and reading is always free, and we plan to keep it that way.
Donate now to our spring fundraiser to help ensure the future of free, accessible literature for all.
—————
To viewers grieving the death of Stranger Things—by death I mean not the finale of the Netflix series this past January, but the show’s unfortunate decline, after the third season, into a plodding, convoluted ghost of its former self—let me offer something of an analgesic. Travel with me, if you will, back to the superb first season, where Winona Ryder’s Joyce Byers, a broke, chain smoking, seemingly delusional mother, opens a can of paint and scrawls the alphabet onto a wall of her home. Joyce hopes her missing son will use the letters to communicate with her from the Beyond. Ryder’s performance would count as one of the most convincing portrayals of insanity in recent screen history, if it weren’t for one thing: Joyce is not mentally ill. Her son is trapped in the Upside Down, and her love is so powerful, she’s able to ignore the rules of logic and perceive what no one else can.
I became a fan of Stranger Things around the time I became, in my own way, Joyce Byers. To certain people in my life, I had recently morphed into a neurotic, monomaniacal woman. Not because I thought my child had been kidnapped by supernatural beings, but because I was convinced I was sick even though no tests could prove it. At 34, during my first year of a doctoral program in literature, I began to experience an electric-shock like pain in my pelvis. Sitting exacerbated the pain, so I bought a standing desk. Exercise beyond walking hurt, so I gave up biking, yoga, and rock climbing. Through regular physical therapy and rest, I managed the pain for several years. Then, in early 2020, my symptoms mysteriously worsened.
By the end of 2020, simply getting out of bed was excruciating. I left my graduate program with my dissertation halfway done. From bed, I booked appointments with a new round of doctors: radiologists, pain specialists, pelvic specialists. Everywhere I turned, practitioners doubted me when I said walking and standing were excruciating. A psychologist whom I was required to see as part of my treatment at a pain clinic asked if my parents had treated me well, hinting the source of my symptoms resided in childhood trauma. In her assessment, she concluded, “Ms. Cutchin has some symptoms and behaviors known to be unhelpful for pain including: some fear, avoidant behavior, pain anxiety.”
When a physical therapist saw me limping, she said, “Ask yourself, ‘Why do I feel I have to walk like this?’”
Worst of all, someone close to me hinted I was unconsciously refusing to walk because I “liked the bed and the bath.”
Holed up in bed—a bed that had become for some a symbol of my mental instability—I began watching science fiction. I’ve long been a fan of murder shows and spy thrillers, series in which the culprits are certifiably human and logic more or less carries the day. I binged The Americans, The Bureau, and Bosch, along with some less illustrious procedurals. Then, for want of new programming—it appeared my pain could outlast even Peak TV’s flood of content—I began to watch sci-fi
Not only did sci-fi keep me entertained; it gave me strength. A recurrent trope of sci-fi is the woman who is not believed. There’s Joyce Byers and her can of paint. Iconically, there’s Sarah Connor (Linda Hamilton) in Terminator 2, locked away in a mental institution because she claims—accurately—that cyborgs from the future want to kill her son. In Robert Zemeckis’s 1997 film Contact, based on the book by Carl Sagan, Ellie Arroway (Jodie Foster) tells a senate committee she traveled through wormholes to meet an alien disguised as her father. The (male) chairman points out that video evidence contradicts her account and accuses her of suffering from a “self-reinforcing delusion.”
Not only did sci-fi keep me entertained; it gave me strength.
Also delusional, or so a male colleague insists, is DCI Rachel Carey (Holliday Grainger) in the excellent near-future dystopian series The Capture. When DCI Carey confronts a superior, Commander Danny Hart (Ben Miles), with her suspicion the UK government is altering CCTV footage in real time using deep-fake AI technology, he wastes no time gaslighting her. “You’ve had a shock tonight, Rachel. Why don’t you get some rest.” If I had a dollar for every time I’ve heard a male character tell a woman she needs some rest, I’d be able to upgrade every streaming subscription to premium. In the German limited series The Signal, it’s a case of “space sickness” that plagues astronaut Paula (Peri Baumeister), or so a dismissive colleague would have her believe. Aboard a space shuttle, Paula hears a signal she knows can only come from aliens. She records the signal, but when she plays the recording for the rest of her team, there’s nothing on the tape. Her (once again, male) colleague, Hadi (Hadi Khanjanpour), who initially heard the signal, too, tells Paula she’s unwell. “Go lie down.”
Riddled with pain, facing disbelief from those around me, the stories of Joyce, Paula, DCI Carey, Ellie Arroway, and Sarah Connor brought me solace, and a shred of hope. I belonged to a genre of female characters who had to fight to be believed. In the worlds these narratives portray, women’s claims are outlandish, otherworldly, weird, and also true. Eventually, each character finds someone who believes her. Sometimes it’s a man, like Jim Hopper (David Harbour) in Stranger Things, who learns to trust Joyce. Sometimes it’s a woman or girl: Paula’s most steadfast advocate in The Signal is her disabled nine-year-old daughter, Charlie (Yuna Bennett), who, working with her father, figures out the time and place of the aliens’ arrival and proves her mother right.
Watching these films and shows between visits to doctors bent on dismissing me, I grasped sci-fi’s genius: It taps into our culture’s deepest anxieties about the trustworthiness of women. In our real-world political climate, when a woman speaks her experience, whether she’s talking about sexual abuse, harassment, or illness, we wonder, Where’s the proof? And yet, our standards of proof are devised by the same systems—legal, educational, medical—built by men to protect male interests. In the medical system, imaging and other tests count as “proof” of illness or pain, but such tests screen only for well-researched diseases, and what we know about those diseases largely comes from research on male subjects. No definitive tests exist for a host of conditions that predominately affect those assigned female at birth, like myalgic encephalomyelitis/chronic fatigue syndrome and Ehlers-Danlos Syndrome. A woman with this kind of disease might as well be telling her doctors: Cyborgs are coming. Aliens have made contact.
By exploring whose testimony counts as reliable, and on what terms, sci-fi provides a template for what ethical philosophers call epistemic justice. “Epistemic” refers to knowledge. In our everyday lives, we convey knowledge to others by sharing our expertise, by relating our experience, and so forth. When a speaker offering knowledge is dismissed because of who they are—a woman, a trans person, a Black or Brown person—they are wronged in their “capacity as a giver of knowledge,” as philosopher Miranda Fricker puts it in Epistemic Injustice: Power and the Ethics of Knowing. The one who speaks loses out, but so does a community of hearers who would benefit from the information the speaker seeks to convey. Sci-fi dramatizes epistemic injustice and proposes a different way: We must practice epistemic humility by taking stock of our prejudices and admitting that someone who looks and sounds different than us might be right.
In the eyes of Western medicine, there is little stranger than a malfunctioning female or gender nonconforming body. According to The New York Times, “Women are more likely to be misdiagnosed than men in a variety of situations.” A stunning 72% of millennial women report feeling gaslit by medical professionals, a Mira survey found. If you’re nonwhite, it gets worse. Black women are less likely to develop breast cancer than white women—but 40% more likely to die from the disease due to delays in diagnosis and care. Delays in diagnosis stem partly from lack of research into women’s health. Until recently, women were considered inferior subjects to men in basically all research. “There are parts of your body less known than the bottom of the ocean, or the surface of mars,” Rachel E. Gross writes in Vagina Obscura: An Anatomical Voyage. On top of it all, there’s medicine’s age-old tendency to see women’s maladies as psychogenic in nature—think of the prevalence of the hysteria diagnosis in the nineteenth and twentieth centuries.
Today, women are less likely to be told our pain or fatigue is “in our heads.” Instead, in a sophistry-laden twist, we are told our symptoms stem from a “brain” gone haywire. According to the brain-based model of chronic pain, when symptoms persist more than three to six months with no obvious organic cause, the brain is at fault, or more precisely, a “maladaptive plastic reorganization in central pain processing circuits.” A spate of recent self-help books and pain reeducation programs promise to teach your brain to unlearn pain via cognitive-behavioral interventions. The problem with these treatments is they fail to account for the instances when pain persists because doctors and tests miss its underlying cause. Around 70% of chronic pain patients are female. Women are more likely to suffer from underreached conditions like fibromyalgia, autoimmune disease, Ehlers-Danlos Syndrome, pelvic pain, Long Covid, Lyme disease, and myalgic encephalomyelitis/chronic fatigue syndrome. Telling a woman her pain stems from a “maladaptive” brain is today’s version of “it’s just hysteria.”
Given sci-fi’s uncanny ability to channel and critique these medical biases, I’ve put together a quiz: Can you tell the difference between a real-life sick woman and science fiction? The following statements were uttered either in a science fiction film or TV show, or in a real-life medical setting where a female patient came in complaining of physical symptoms. Circle the correct answer:
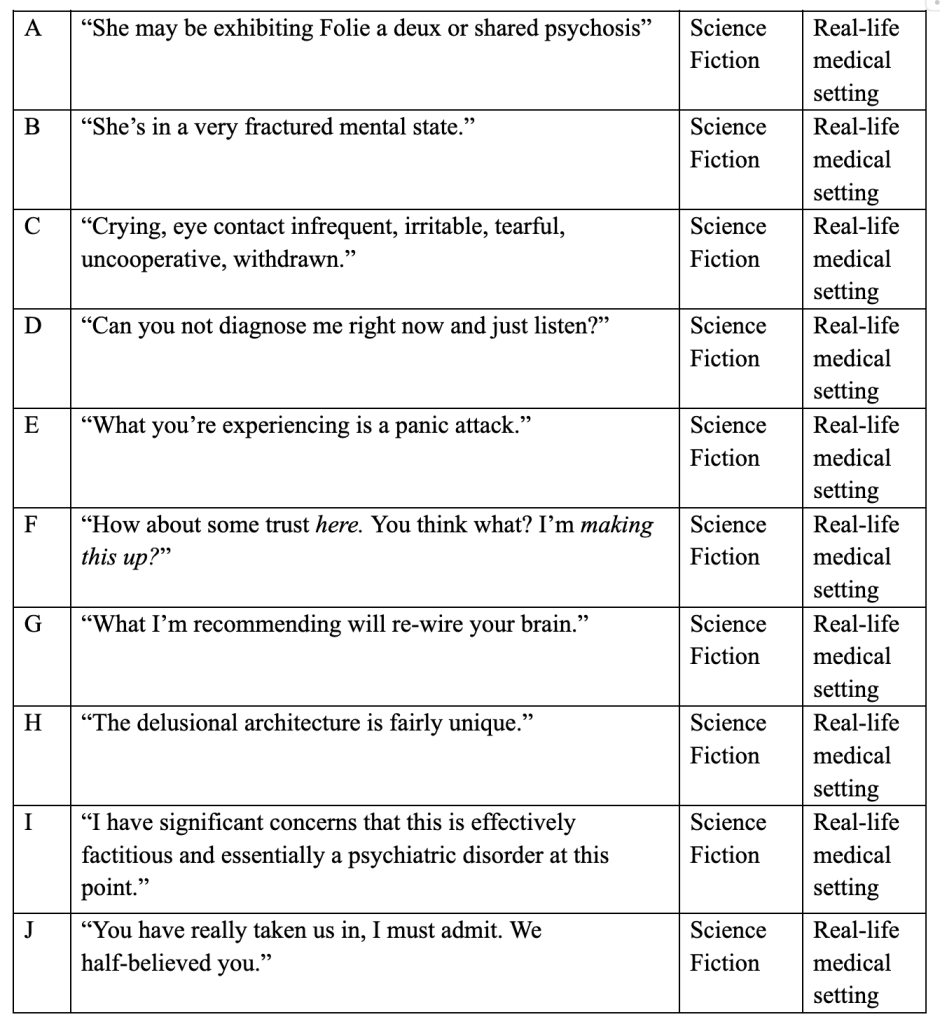
Answer key: B, D, F, H and J are from science fiction—The OA, Manifest, Stranger Things, Terminator 2, and The Lion, the Witch, and the Wardrobe, respectively. A, C and I are from medical records shared with me by a female patient with Ehlers-Danlos Syndrome; E was uttered by the doctor of an Instagram user living with ME/CFS and POTS. G is from my own life. A noted Bay Area pelvic pain practitioner insisted I download a pain therapy app that could, he said, “re-wire” my brain so I no longer felt pain. “The app will teach you that you can’t use the word ‘pain’ any longer if you want to heal,” he told me.
I’m not saying mind-body tools aren’t helpful in managing symptoms. In the early years of my pain, I did quite a lot of psychotherapy and embodied meditation. These tools helped, especially when it came to managing the stress of illness. By the time I became bedridden, I knew I’d gone as far as I could with mind-body modalities. I told anyone who would listen I believed my symptoms had a biomechanical source, but, as time went on, I doubted that source would ever be found. After all, I’d had an MRI, the gold standard for diagnosis of pelvic disorders, and it had revealed nothing.
Still, I kept searching. For years, I’d been hearing about a world-famous pelvic pain specialist in Arizona. Seeing him would mean traveling seven hundred miles and paying for the visit out of pocket. By early 2022, I was out of other options. A friend and I rented a van and drove seven hundred miles from our home in the San Francisco Bay Area into the Arizona desert listening to crime podcasts. Actually, my friend drove; I laid on a mattress in the back.
The Arizona doctor took by far the most careful, thorough patient history of any provider I’d seen. He recommended a round of pelvic floor botox, and, when that didn’t work, he offered a diagnosis.
When a woman speaks her experience, whether she’s talking about sexual abuse, harassment, or illness, we wonder, Where’s the proof?
“All the signs point to pudendal nerve entrapment.”
The pudendal nerve runs through the lower pelvis and innervates urinary, bowel, and sexual function. I’d long known my nerve was irritated. But none of the pelvic specialists I’d seen had raised the possibility it might be compressed. Compression, the Arizona doctor explained, doesn’t show up on an MRI; the nerve is too small, too hidden. Compression typically arises from a traumatic injury, or repetitive stress. The year before the onset of my symptoms, I’d biked one thousand miles down the California coast. The pressure of the bike seat against my pelvis caused scar tissue to build up around the nerve. To protect the nerve, paradoxically.
It took 11 years from the onset of symptoms to receive the diagnosis. The treatment: a fairly straightforward decompression surgery.
Pudendal nerve entrapment is an underresearched condition that affects—you guessed it—women more often than men at a rate of seven to three. Childbirth is a common trigger. Diagnostic criteria do exist, but none of the chronic pain or pelvic disorder specialists I’d previously seen were familiar with those criteria. Pudendal entrapment isn’t common, but it’s not as rare as one might think, either. Studies indicate it affects up to one percent of the general population. Because pudendal entrapment lacks an ICD-code—such codes are used globally to classify medical diagnosess—insurance companies view decompression surgery as experimental and refuse to reimburse it. (In contrast, ICD-codes exist for “Sucked into jet engine V97.33X” and “Struck by turkey W61.42XA.”)
Four months after surgery, I began to see improvement. Within 15 months, I was leading a normal life again: walking, sitting, and traveling—without a van and mattress. I made plans to return to the PhD program.
Today, I’m grateful to the Arizona doctor who took the time to listen and believe my story. I’m also, frankly, enraged when I think about the time, energy, and pain I would have been spared if the medical system had the patience and trust to take my symptoms seriously. If it had, I wouldn’t have become Joyce Beyers and spent years getting others to see the writing on the wall.

